Nephrostomies are inserted when there is an obstruction to the normal drainage of urine from the renal tract or to divert urine flow from a leak/anastomosis.
The nephrostomy is inserted under ultrasound and fluoroscopic guidance, the pigtail of the nephrostomy usually within the renal pelvis.
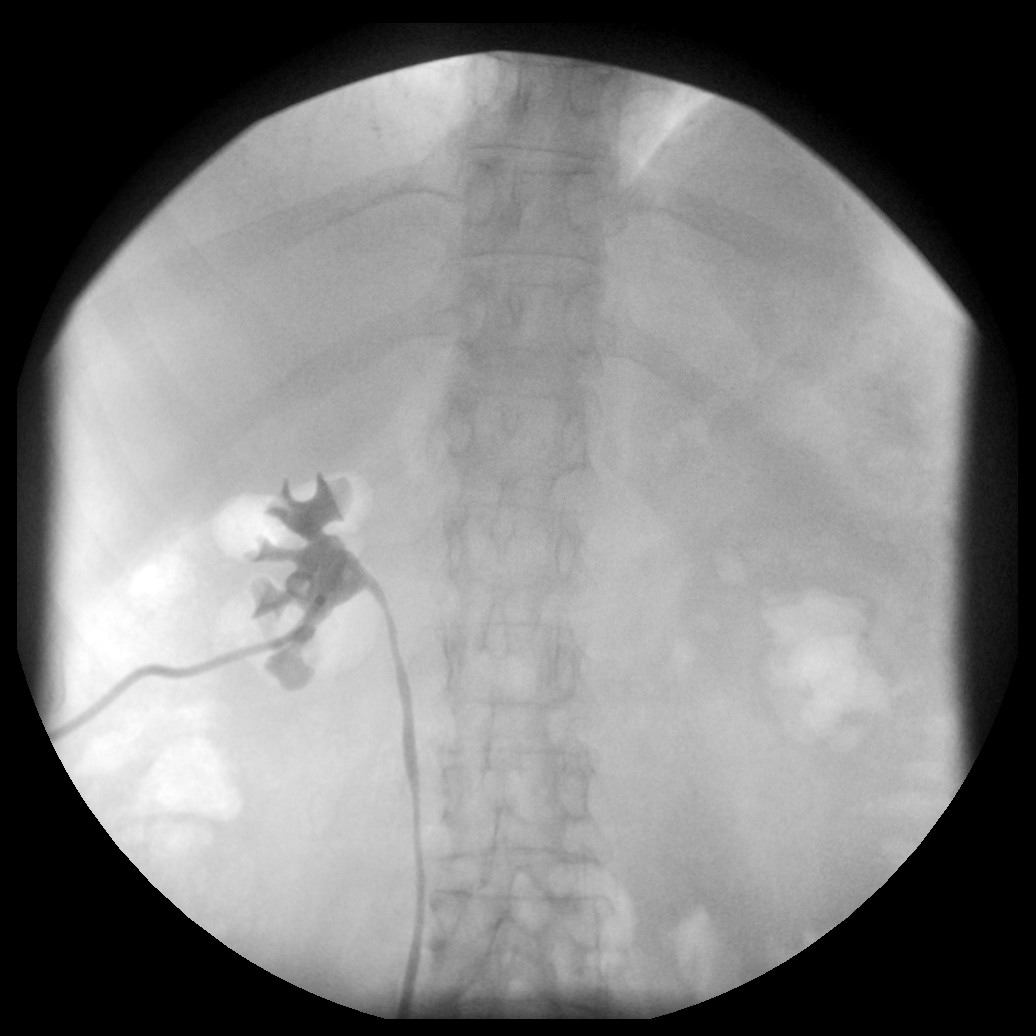
Prone image of a normally sited L nephrostomy within the renal pelvis

The clinical indication for a nephrostogram may include:
nephrostomy has stopped draining: is it in the correct place?
pain around nephrostomy site: is it in the correct place or leaking?
is there a leak from a distally surgical anastomosis or urinary diversion?
to review whether there is still an obstruction or if the obstruction (stone) has moved
to investigate the cause of obstruction
post PCNL to check for residual stones or leak
This clinical information is vital so you know where to look and what to look for.
Transplant nephrostograms can be quite difficult and some of these are best done in the angio suite due to better image quality, complex anatomy and the fact that we will already know the case.

Equipment
Sterile pack, chlorhexadine, sterile drape/sheet, 20ml syringe x 2, saline, contrast (niopam)
Procedure
This is a sterile procedure.
This examination is usually performed with NIOPAM 300 as the contrast medium
The patient is usually positioned supine in the barium suite. In angio most nephrostomies and nephrostograms are performed prone. Ureteric drainage may improve in the prone position. Providing you label which kidney is being imaged the positioning usually doesn’t matter

Check to make sure there is no obvious external kink in the tubing. This is particularly important if the tube is blocked. It may simply be due to a kink. You may need to carefully remove the outer dressing to inspect the tube. If removed it needs replacing.
Take the control film showing the nephrostomy and location of the ureter if required. The control film will be guided by the indication, site of nephrostomy and or stent. If the control film needs to include the entire kidney and ureter then you may be better taking 2 or 3 detailed control rather than 1 poor overview. Remember stones can move both distally and proximally.

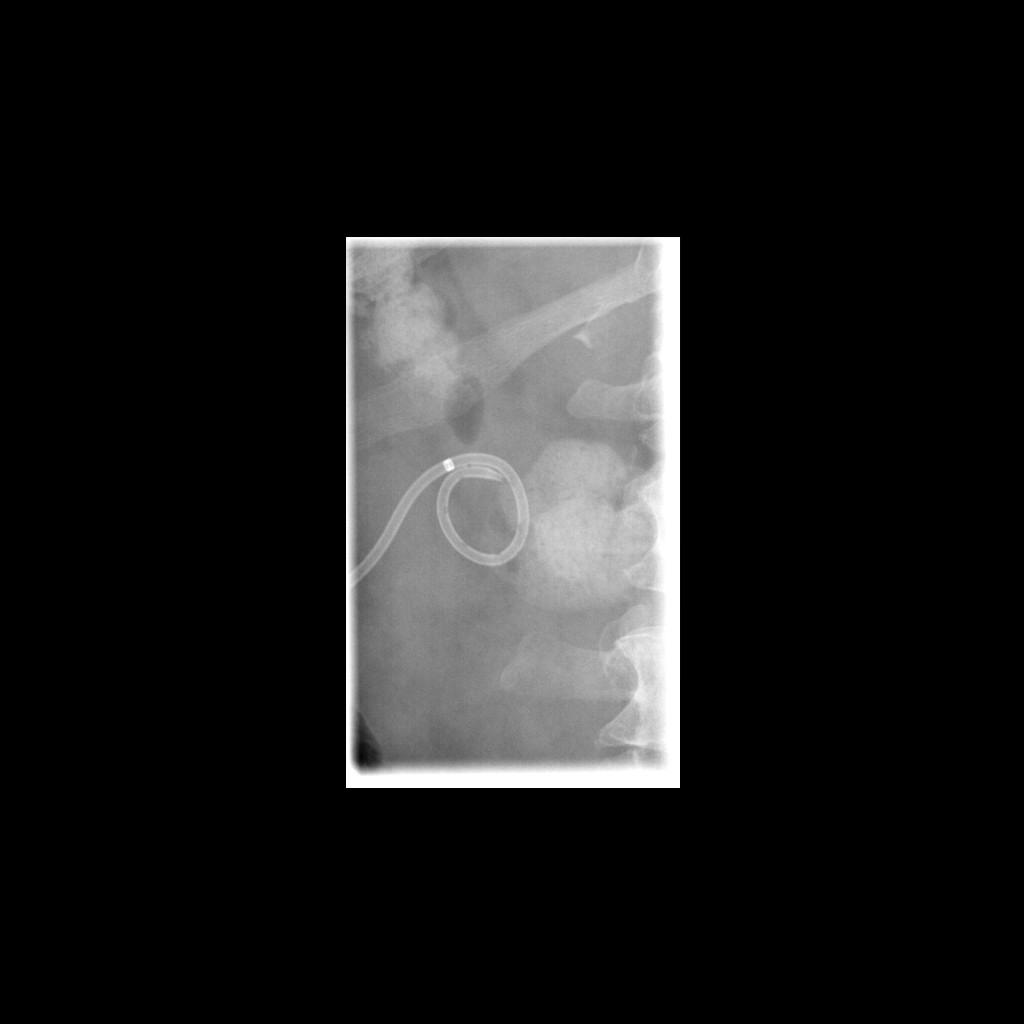
Control film of nephrostomy. Note normal configuration of pigtail drain
Control film overview (nb the VUJ has not been included and another control film of this should be taken)

Clean the nephrostomy with chlorhexadine and use a sterile drape
Gently aspirate to see if urine drains and flush with small volume of saline. Observe the nature of the urine (clear, cloudy, haematuria, purulent). If purulent urine, flush out the system and ensure the patient has or does receive antibiotics and take care in this instance not to over distend the system as a bacteraemia can be caused.
Attach a syringe filled with NIOPAM. Ensure no air bubbles are introduced as they mimic calculi.
Start to inject contrast under fluoroscopic screening
Screen as the renal calyces begin to opacify, take sequential exposures to demonstrate the renal anatomy, tube position, ureteric anatomy and leaks as necessary
As with all fluoroscopic examinations, early pictures are usually important.
Use fluoroscopy to identify and adjust your radiography and take proper exposures to illustrate detail
Use fluoro frame grabs for dynamic ureteric jets or peristalsis that you are unable to capture on an exposure.
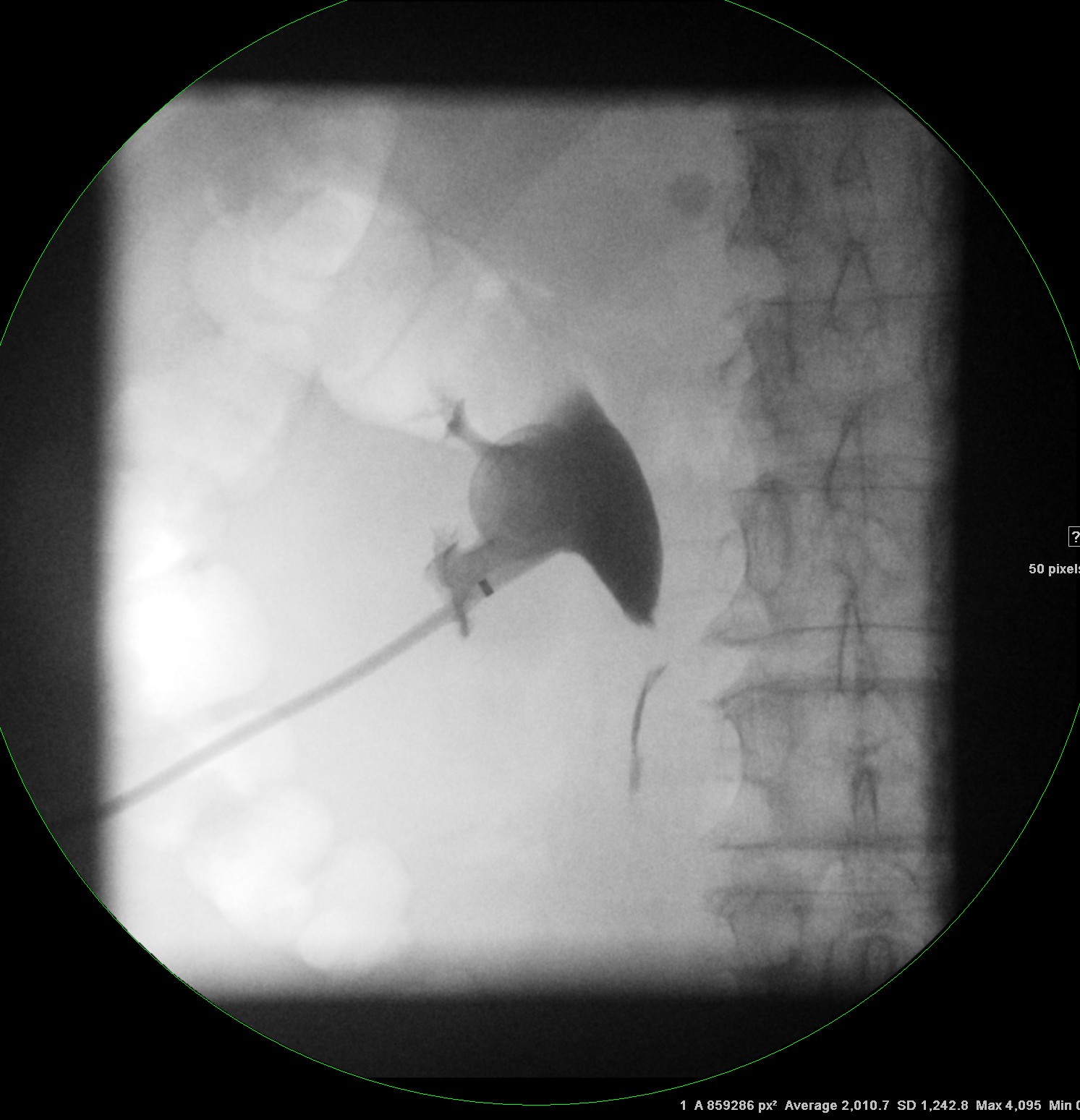
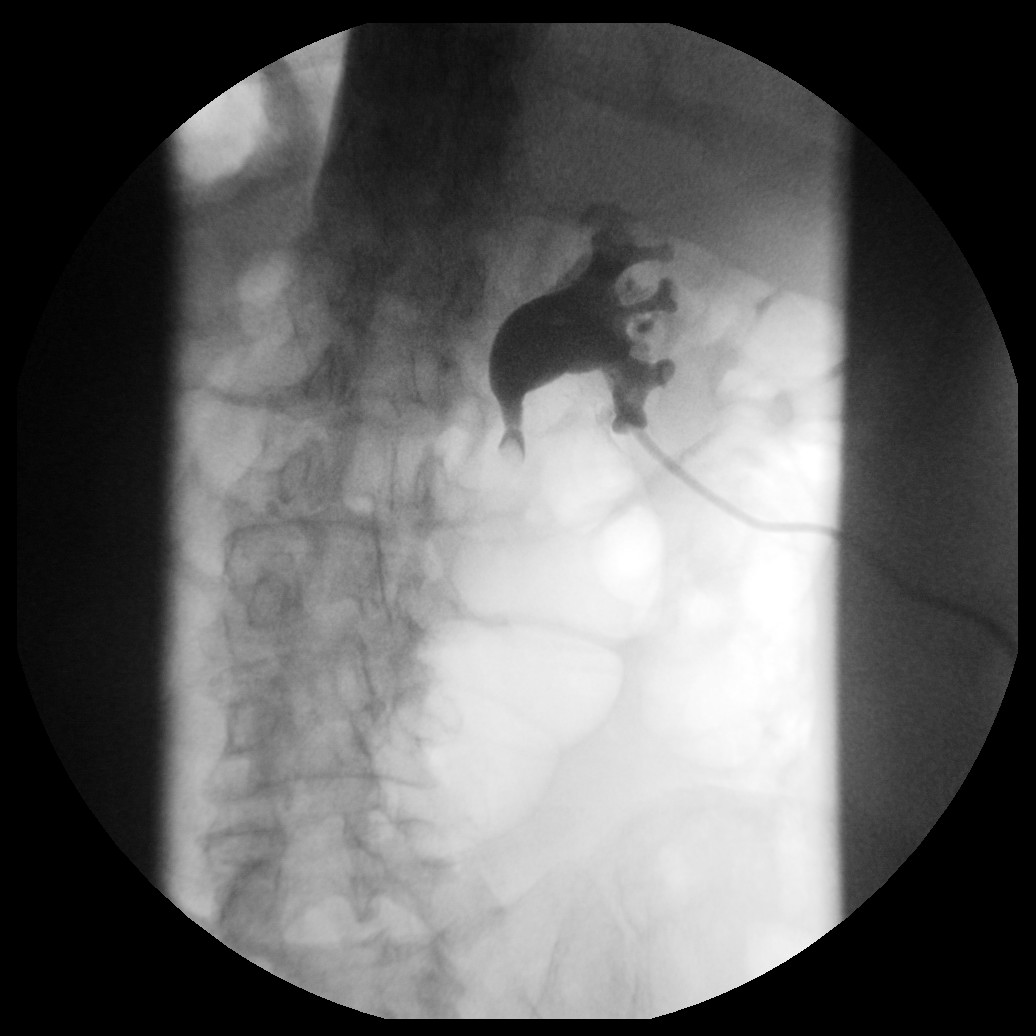
Nephrostomy correctly sited with proximal ureter visualised
If the nephrostomy is in the correct place the calyces should opacify and you may see contrast medium entering and passing distally along the ureter.
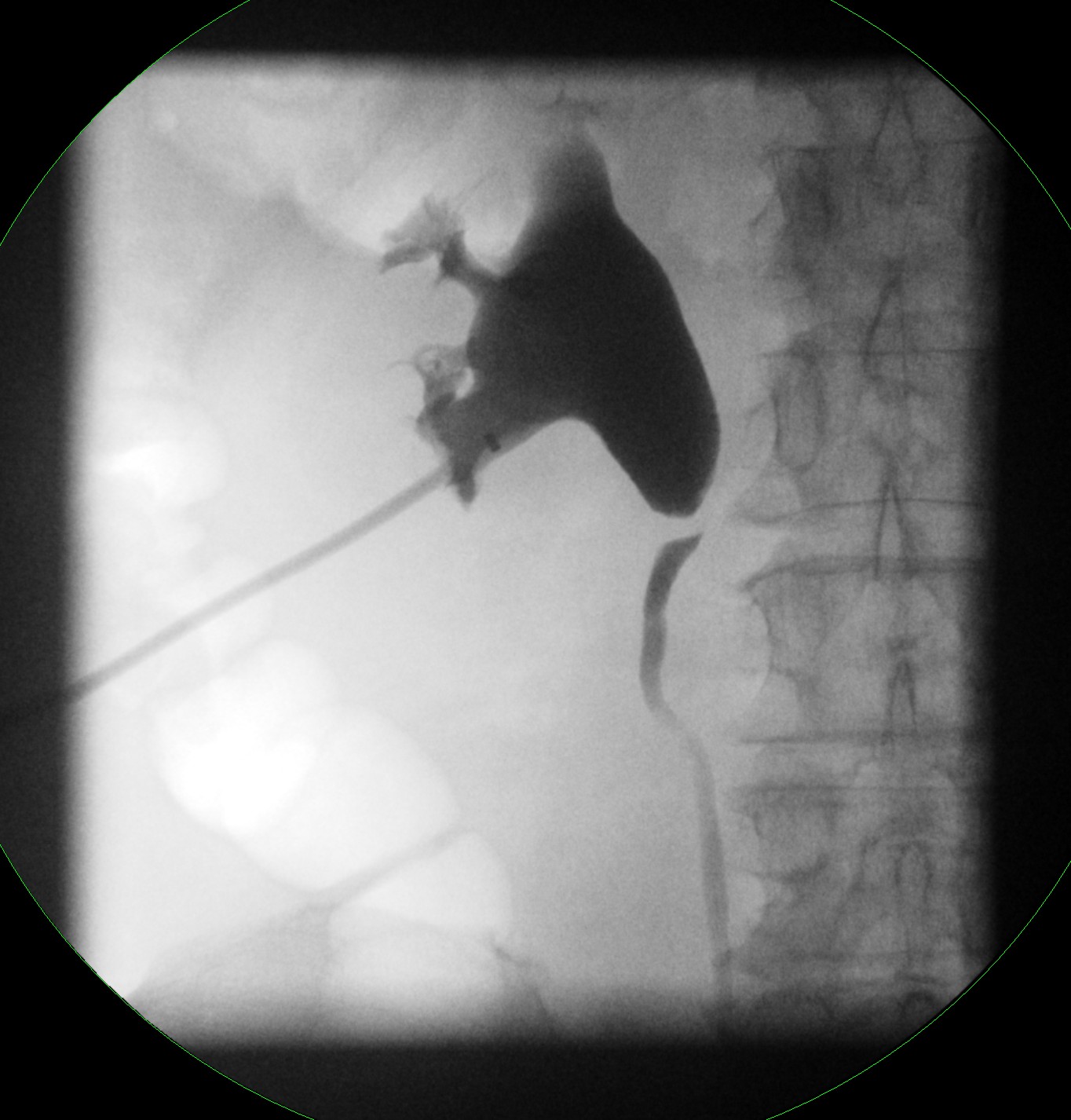
If indicated opacify the ureter and image
The VUJ usually needs magnified views.
Fluoroscopy frame grab images can be useful for demonstrating regions of distended ureter and ureteric jets into the bladder that you cannot capture on exposures.

Aspirate the contrast on completion and reattach the drainage bag or close the nephrostomy as required.
You must annotate your images e.g. left, right, prone, supine, RAO LAO, control, post aspiration. If a patient has bilateral tubes in, mistakes can easily be made as intervention is performed in a prone position but some nephrostograms are done supine!

Make sure the image is processed appropriately a nephrostogram is NEPHG not NEPHR which is a nephrostomy. Even if the wrong code is requested it is your job to do the correct examination and record it correctly.
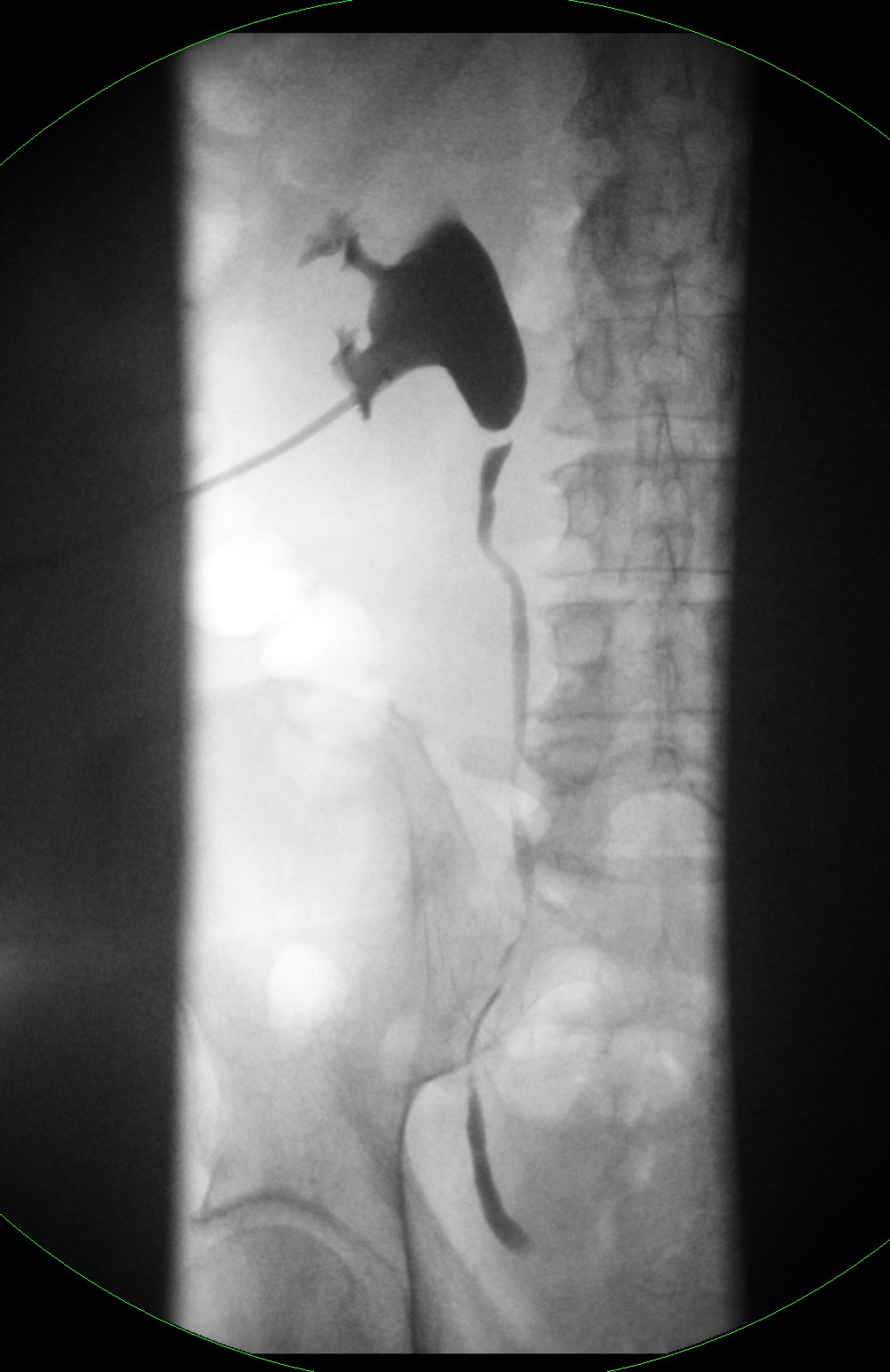
Remember the ureter peristalses normally so you may not see the entire ureter filled on a single image.
Also gravity will fill the dependent calyces (remember there are anterior and posterior calyces)
You will find in certain circumstances that you cannot get all information onto 1 image therefore don’t be afraid to magnify in and get several good quality images that sequentially show what you need
Here are the remainder of the images from the above study.
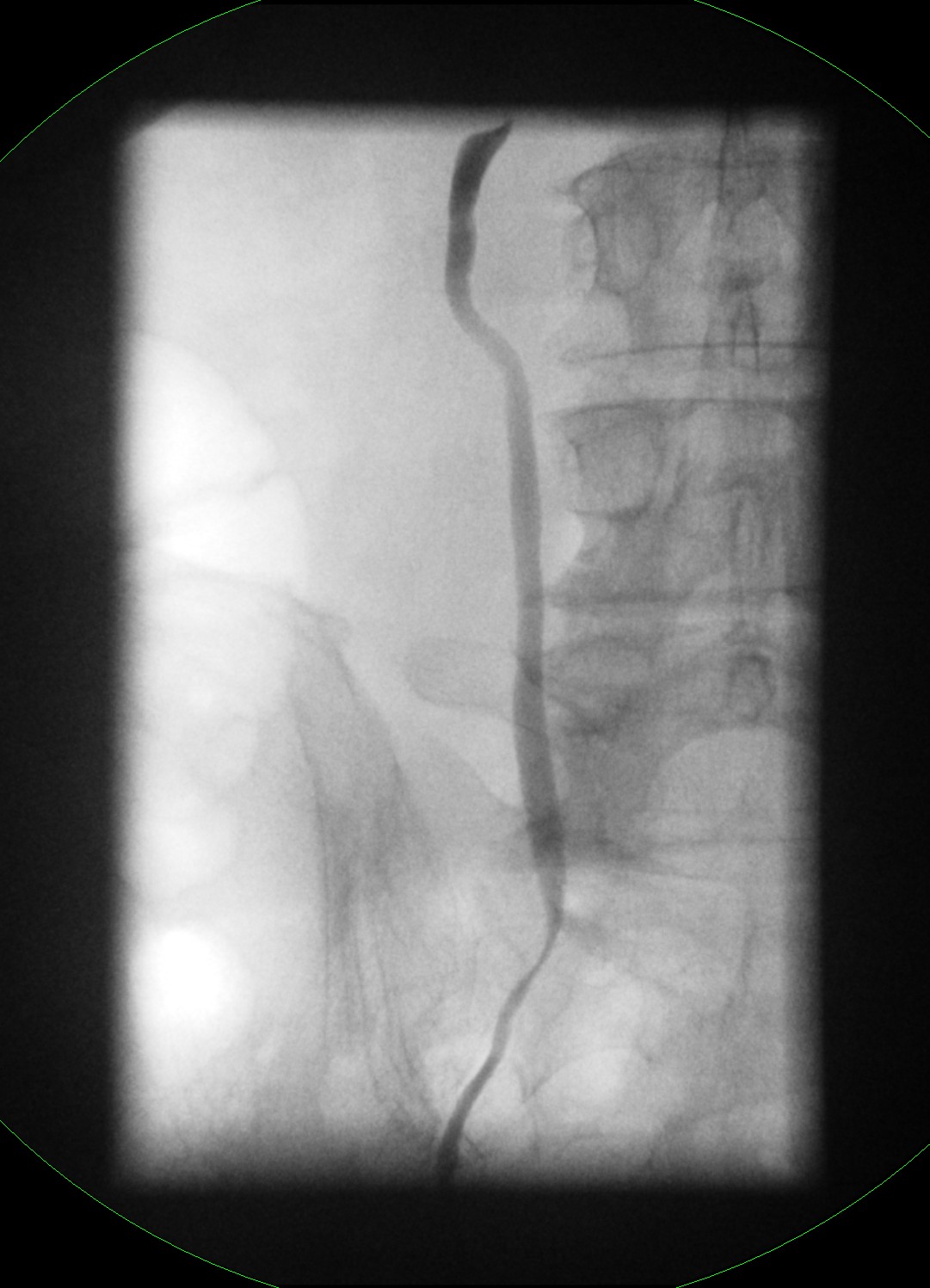
Mid ureter Distal ureter
Bladder jet Overview of whole ureter
Hints and tips:
1 poor overview image with bits missing
Poor centring, magnification and coning DON’T TAKE PICTURES LIKE THIS
A magnified view would have demonstrated this obstructing ureteric calculus much better.
Transplant nephrostograms:
The anatomy of renal transplants is usually standard with the donor ureter reimplated into the native bladder. A ureteric stent is left in situ in the post operative period. However, when there have been problems things can get more complex. If ureteric revision has been performed, then the native ureter is often reattached to the renal transplant pelvis and donor ureter left in situ, hence two ureters. In this scenario, you may have a nephrostomy tube, 2 ureters, 1 stent and sometimes a drainage tube within a urinoma. Clear knowledge of the case is essential prior to imaging or you will find yourself in a mess! If required to image a transplant in barium, make sure to discuss this case carefully to avoid confusion.
The same principles for technique as above apply.
Normal transplant nephrostogram
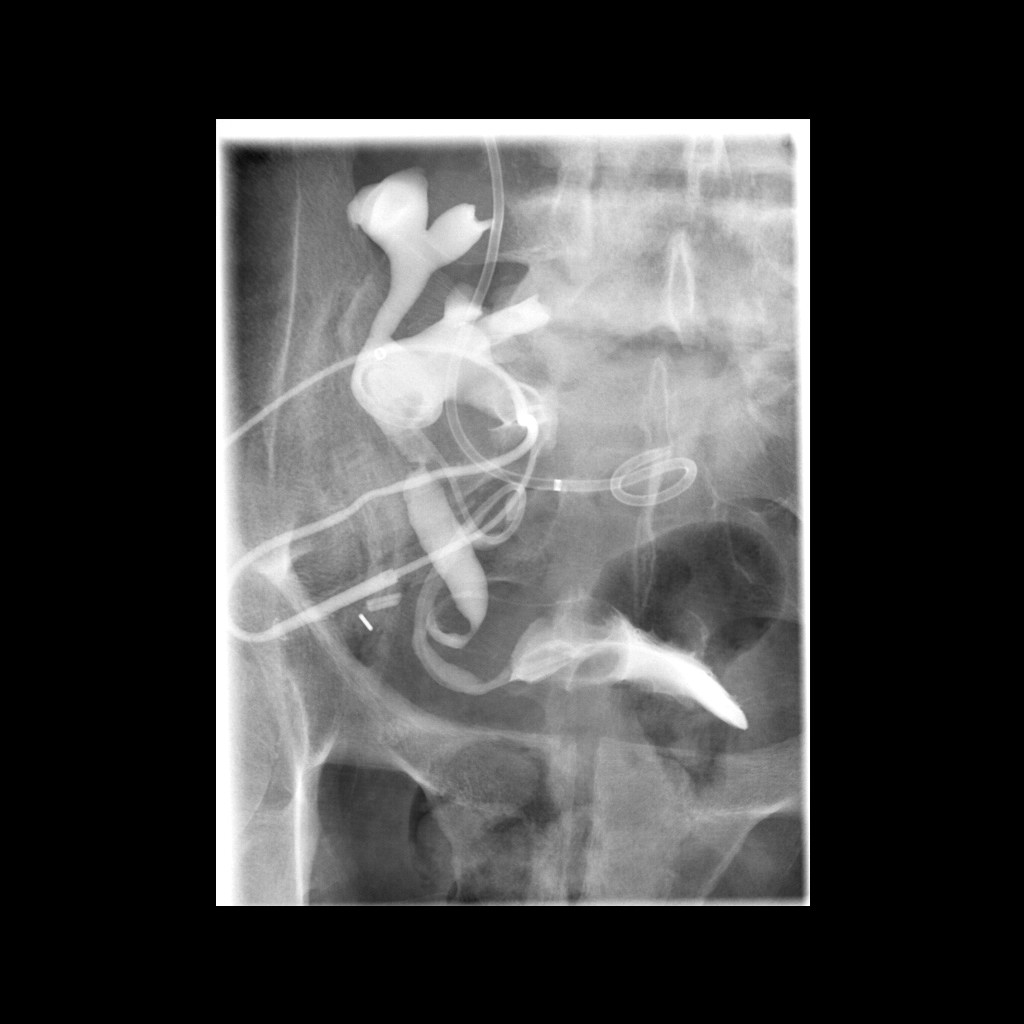
Not all cases are as simple as above and it can get quite difficult.
2 separate transplant nephrostograms. Although complicated they both answer the clinical question